
Vitamin D – or “The Big D” as it’s referred to – continues to garner considerable interest in the scientific/medical community, and for good reason. I’m not going to cover all the potential benefits of this vitamin in this article, as that information exists all through this site and a topic I and other authors – namely Monica Mollica – have been covering for years now. In terms of a summary of benefits and how to optimize doses and other essential aspects of D, her article on that topic is a ‘must read’ and found HERE.
Vitamin D has been receiving yet more attention recently due to it’s association with Covid; several studies finding strong correlation between vitamin D status and serious complications and mortality rates from that virus. I discuss that topic as it applies to what may be the missing link in the high mortality rates in African American’s and Covid HERE.
This write up I want to focus on what is a key aspect for getting the most from Vitamin D, with a focus on those who have failed to bring their 25(OH)D numbers up even while taking high doses of D3.
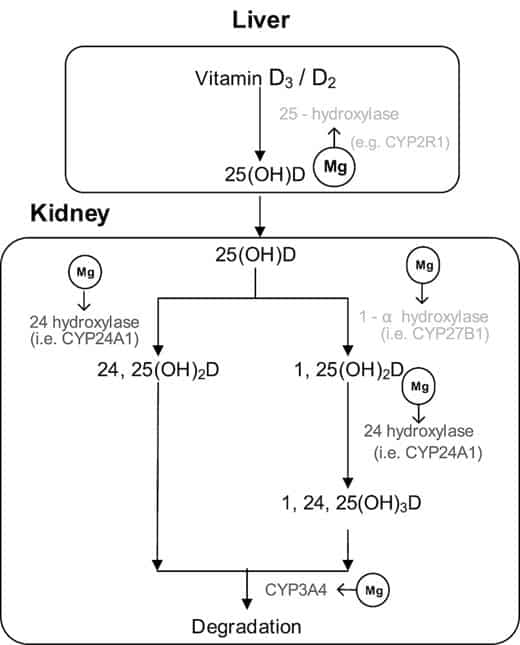
In a nut shell: Magnesium is an essential co-factor for the enzymes that produce the various biologically active downstream metabolites of D3 and magnesium deficiencies are very common in the US population, estimated to be approximately 80% of the population. Due to food production methods and other factors, the mag/calcium ratios are not what they should be in our diets, and getting adequate magnesium via food sources without additional supplementation is quite difficult, bordering on impossible… A ground breaking study below found supplemental magnesium had profound effects on vitamin D metabolism.
Over the years I have marveled at the doses of D3 people would take and see minimal to no impacts on their 25(OH)D levels, and it’s quite possible that’s been due to their magnesium status. Magnesium plays a central role in D metabolism and that some are resistant to vitamin D therapy, their magnesium status may be, at least in part, responsible for it. As magnesium deficiencies are common, and the mineral essential for over 300 different enzymes to function in the human body, and is associated with a long list of benefits to human health, I view a magnesium supplement a “no brainer” to include at this point.
Magnesium Citrate has good data and relatively inexpensive although other forms exist. Per above, magnesium is one of the few “no brainer” supplements in my view, and of course people should also attempt to focus on magnesium rich food sources (e.g., “green leafy vegetables, legumes, whole grains, seeds, and nuts as good sources…” ) in their diets. If you’re one of those people who find they’re able to take high doses of D3 with minimal to no impact on 25(OH)D levels, it may be due to your magnesium status and that would be the first place I’d look to address the issue.
Magnesium status and supplementation influence vitamin D status and metabolism: results from a randomized trial
The American Journal of Clinical Nutrition, Volume 108, Issue 6, December 2018, Pages 1249–1258
ABSTRACT
Background
Previous in vitro and in vivo studies indicate that enzymes that synthesize and metabolize vitamin D are magnesium dependent. Recent observational studies found that magnesium intake significantly interacted with vitamin D in relation to vitamin D status and risk of mortality. According to NHANES, 79% of US adults do not meet their Recommended Dietary Allowance of magnesium.
Objectives
The aim of this study was to test the hypothesis that magnesium supplementation differentially affects vitamin D metabolism dependent on baseline 25-hydroxyvitamin D [25(OH)D] concentration.
Methods
The study included 180 participants aged 40–85 y and is a National Cancer Institute independently funded ancillary study, nested within the Personalized Prevention of Colorectal Cancer Trial (PPCCT), which enrolled 250 participants. The PPCCT is a double-blind 2 × 2 factorial randomized controlled trial conducted in the Vanderbilt University Medical Center. Doses for both magnesium and placebo were customized based on baseline dietary intakes. Subjects were randomly assigned to treatments using a permuted-block randomization algorithm. Changes in plasma 25-hydroxyvitamin D3 [25(OH)D3], 25-hydroxyvitamin D2 [25(OH)D2], 1,25-dihydroxyvitamin D3, 1,25-dihydroxyvitamin D2, and 24,25-dihydroxyvitamin D3 [24,25(OH)2D3] were measured by liquid chromatography–mass spectrometry.
Results
The relations between magnesium treatment and plasma concentrations of 25(OH)D3, 25(OH)D2, and 24,25(OH)2D3 were significantly different dependent on the baseline concentrations of 25(OH)D, and significant interactions persisted after Bonferroni corrections. Magnesium supplementation increased the 25(OH)D3 concentration when baseline 25(OH)D concentrations were close to 30 ng/mL, but decreased it when baseline 25(OH)D was higher (from ∼30 to 50 ng/mL). Magnesium treatment significantly affected 24,25(OH)2D3 concentration when baseline 25(OH)D concentration was 50 ng/mL but not 30 ng/mL. On the other hand, magnesium treatment increased 25(OH)D2 as baseline 25(OH)D increased.
Conclusion
Our findings suggest that optimal magnesium status may be important for optimizing 25(OH)D status.
Will Brink is the owner of the Brinkzone Blog. Will has over 30 years experience as a respected author, columnist and consultant, to the supplement, fitness, bodybuilding, and weight loss industry and has been extensively published. Will graduated from Harvard University with a concentration in the natural sciences, and is a consultant to major supplement, dairy, and pharmaceutical companies.
His often ground breaking articles can be found in publications such as Lets Live, Muscle Media 2000, MuscleMag International, The Life Extension Magazine, Muscle n Fitness, Inside Karate, Exercise For Men Only, Body International, Power, Oxygen, Penthouse, Women’s World and The Townsend Letter For Doctors.
He’s also been published in peer reviewed journals.
Will is the author of the popular e-books, both accompanied by private members forum access , Bodybuilding Revealed & Fat Loss Revealed.
You can also buy Will’s other books on Amazon, Apple iBook, and Barnes and Noble.




{kind=link}
I take around 7000 vitamin D3@ day. I also take magnesium in my bone supplement. Do hospitals still give patients D3 as one of first lines of defenses? Love your articles. They have been so good lately that I have sent them on to my daughters who love this factual information.
Hospitals don’t give any supplements as a first line defense, so not sure what you mean by “still” on that one.
So what’s the dosage for Magnesium in a supplement to help with D3?
It would be IV. Not as “supplement”
No, not IV. No idea where you’re getting that from but it’s not accurate.
I think what they may be referring to is a radio info commercial for Purity Products that features Dr. John Cannell. In this radio spot he makes the statement something like “if you went to the emergency room with a suspected heart condition the very first thing they would give you was 100,000 iu’s of Vitamin D3”. I am not saying this because I believe it ,but you wondered where the last couple of comments got this from. This may be the source of those comments.
I’d love to see his source on that one…
Will, does the Magnesium need to be taken at the same time as the D3? I do supplement with Life Extension Neuro-Mag nightly (L-Threonate) nightly, but don’t take it with my D3 (morning).
Thanks,
You don’t need to take them together. Mg doses discussed in the vid, and tweak as needed.
excellent mr. bill, stay safe,.