The mere word cholesterol gives many goose bumps. We have been indoctrinated since the well-known Framingham Studies that the higher the blood cholesterol level, the higher the risk of heart disease 1-3. However, much has been discovered in medical research since then. Today there is compelling evidence showing that strict reliance on the traditional cholesterol test that is routinely run in the clinic can falsely tell you and your doctor that you’re fine, even if you aren’t. Here you will find out what to look for…
The traditional cholesterol test
Unless you have a good doctor who keep tabs on medical research, when you do your blood work (which I hope you do regularly as a preventive measure), the traditional cholesterol test that’s part of a regular health check will only give you information on the following measurements:
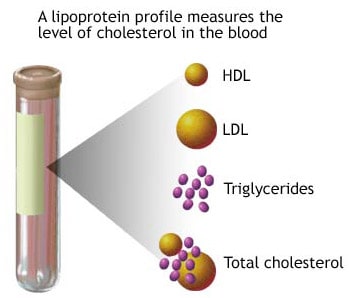 – Total cholesterol level
– Total cholesterol level
– LDL (low-density lipoprotein, the “bad” cholesterol)
– HDL (high-density lipoprotein, the “good” cholesterol)
– Triglycerides (aka blood fats)
This traditional cholesterol test is also called the standard lipid panel. Lipid is a catch-all term for fats and cholesterol, which are characterized by their water insolubility. Hence the need for lipoproteins, which are molecules that transport cholesterol and fats in the blood. Blood cholesterol gets its name based on what particle that carries it in the blood stream. Even though you often hear discussions about bad and good cholesterol, the cholesterol in LDL and HDL is the same; the difference lies in their respective transport molecule (ie, the lipoproteins).
Doctors have historically blindly relied on this standard lipid panel (traditional cholesterol test) to assess their patients’ risk of cardiovascular disease and prescribe cholesterol lowering drugs. However, there are serious limitations in relying solely on the standard cholesterol panel. Most importantly, it can identify only about 40% of people at risk for coronary heart disease 4, and the extent of cardiovascular disease varies greatly among individuals with similar “standard” cholesterol levels 5,6. Over the past decade, an immense amount of scientific research has shown that within each cholesterol class (LDL, HDL etc) distinct subclasses exist, that confer different degrees of cardiovascular disease risk 7. For example, it is the small LDL particles that are dangerous, and not so much the larger LDL particles 8-10. This discovery has given rise to the “pattern A” and “pattern B” notations (see below) and explains why a simple total LDL level test doesn’t tell you the full story and can be misleading.
VAP – the next generation of cholesterol testing
The VAP (Vertical Auto Profile) test provides this valuable information on cholesterol/lipoprotein subclasses. The expanded information from the VAP test includes:
– More accurate, direct measurement of LDL:
The standard lipid panel only indirectly gets your LDL level by a calculation, which is fraught with questionable assumptions 11-13.
– Measurement of LDL particle number and density:
This is important because small, dense and numerous LDL particles (“Pattern B”, see below) cause a 3-fold increase in risk of a heart attack independent of the total LDL level 9,14.
– Measurement of lipoprotein subclasses and related molecules.
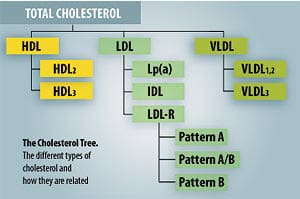
This includes, LDL1, LDL2 and LDL3, HDL2 and HDL3, intermediate-density lipoprotein (IDL), very-low-density lipoproteins (VLDL1, VLDL2, VLDL3), and lipoprotein(a) [ Lp(a) ], a particularly dangerous lipoprotein that can lead to heart attacks and strokes. The VAP test will also give your apo-B level; apo-B is a molecule that is attached to each LDL particle, and gives another dimension of your LDL particle number.
People who test “normal” in a standard cholesterol test often are found to be at risk for heart disease after taking the VAP test. This is because individuals with the same LDL level may have high or low numbers of LDL particles. Because LDL particle number is an independent and more sensitive indicator of risk than LDL (or non-HDL), these individuals will differ in terms of heart disease and cardiovascular risk, despite having same LDL level 8,15. This is clearly of utmost importance, for both prevention and treatment.
Nail down you LDL pattern – are you an A or B?
When you get your VAP results, all the numbers can make you dizzy. No worry, the main thing to find out is your LDL pattern. The LDL patterns A and B refer to the size of LDL cholesterol particles in the blood.
Persons with LDL pattern A have large, buoyant LDL particles. Individuals with pattern A are more likely to have normal blood levels of HDL and triglycerides. Pattern A is usually not associated with cardiovascular risk.
Persons with LDL pattern B have predominantly small and dense LDL particles. Pattern B is frequently associated with low HDL levels, elevated triglyceride levels, and high blood sugar levels and risk for type II diabetes. Individuals with pattern B are also more likely to develop high blood triglyceride levels after a fat-rich meal (a medical condition called postprandial hyperlipidemia).
Why is this important?
Smaller LDL particles are more dangerous than the larger ones because they can more easily squeeze through the endothelium (a single cell layer that lines blood vessels) and clog up the artery walls. Smaller LDL particles also are more easily oxidized, and oxidized LDL is a significant contributor to the formation of plaques in the arteries.
More and more scientific medical research is showing that the total LDL level is not the best indicator of heart disease risk that has been attributed to LDL. The reason for this is that the risk correlates more strongly with the number of circulating atherogenic LDL particles (as can be found out in a VAP test) rather than the quantity of cholesterol carried by those particles (as shown in a standard lipid panel test) 16. If this is over your head, don’t fret; just make sure you’re a pattern A. And that’s easy because the VAP results page tell you right upfront what pattern you are, so you don’t have to do any calculations. 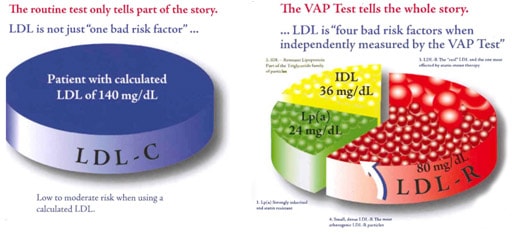
As you can see in the nearby graphic, the LDL fraction is further split into four parts; small LDL particles, large LDL particle, Lp(a) and IDL. Other than telling you whether you are an A or B (ie, whether you have a predominance of dangerous small or less dangerous large LDL particles), the VAP test report also informs you on your standing with these other variables.
Where can I get the VAP test?
If you don’t have health insurance, or if your insurance doesn’t cover it, you can easily order a VAP test for $90 from Life Extension:
VAP™ Blood Test
Here’s an explanation of all the variables you find on the VAP test
Here you can check out a sample VAP report
Other similar advance blood lipid tests
In this article I’ve covered the VAP test from Atherotec, www.thevaptest.com, which is based on the ultracentrifugation technique.
There are also other, similar advanced lipid test available. The most notable is the one based on the nuclear magnetic resonance (NMR) technique from LipoScience, www.lipoprofile.com.
Then we have a gradient gel electrophoresis based test, from Berkeley HeartLab, www.bhlinc.com, and another one based on the ion mobility technique. Since this is an intense research area, we can expect to hear about new advanced lipid test in the near future.
The point I want to make is that, unless your doctor order a specific advanced lipid test for you (buy him/her flowers if that’s the case!), pick one and stick to it. The reason being that the different tests can give you different readings. Thus, you cannot directly compare your VAP reading with an NMR reading if you do both.
You should to do your advanced lipid testing not just once, but regularly to monitor your health status, and effectiveness of your diet and exercise program etc. As of this writing, the VAP test is cheapest.
Who should you care about getting the advanced VAP cholesterol test?
Everybody! Prevention is key for healthy longevity. The “good” thing with cardiovascular disease risk factors is that if you detect them at an early stage, you can easily fix them with diet and exercise, and thereby avoid becoming a victim for heart disease, which is still the number one killer.
If your standard lipid panel shows that you have a high triglyceride level, and/or a low HDL level, you definitely should get the VAP test, since a high ratio of triglyceride/HDL is often accompanied by small LDL particle sizes 17,18. Another simple way to tell is you could be at risk is if you have a belly fat. Having a belly is not just an esthetic issue, it is also a great health risk that should be taken very seriously.
Another important indication that you should have a VAP test, is if are on statins. I am not going to get into the evils of statins here. For the purpose of this article, I just want to inform you that they are the most lucrative drug ever developed by the pharma industry, and unfortunately the first-line drug prescribed by cardiologist to treat high LDL levels. The reason you have to do a VAP test if you are on statins is that statis lower your overall LDL level more than they lower your LDL particle number 19. Thus, statins can lower your LDL level to the normal range, but still leave you with lots of deleterious LDL particles, and thereby falsely give an indication of a successful treatment. Therefore, if your doctor is only monitoring your overall LDL level while prescribing you statins, get another doctor.
Also, if you are eating loads of carbs, you definitely should have a VAP done, because it is well-documented that a high-carb diet has detrimental effects on cardiovascular risk factors. Among other things, eating lots of carbs increases both your blood fats (triglycerides) and your number of small deleterious LDL particles 20-24.
In addition, certain health promoting supplements can actually elevate your total and LDL cholesterol levels, while beneficially affect your LDL particle distribution. Notable examples are fish oil and algae oil supplements 25,26. By getting your VAP test you have your back covered if you start taking fish oil and your doctor starts pulling his hair because your LDL level has increased.
While financial investments can be risky, investing in your own health is totally risk free. And on top of that it gives you an invaluable return; health, happiness and longevity!
Get your VAP™ Blood Test now!
———————————————————————————————————————————————–
About Monica Mollica > www.Ageless.Fitness

Monica Mollica holds a Master degree in Nutrition from the University of Stockholm / Karolinska Institue, Sweden. She has also done PhD level course work at renowned Baylor University, TX.
Having lost her father in a lifestyle-induced heart attack at an age of 48, she is a strong advocate of primary prevention and early intervention, and the development of lifestyle habits for health promotion at all ages.
Today, Monica is sharing her solid medical research insights, real life hands on experience, and passion for health and fitness by offering nutrition / supplementation / exercise / health consultation services, and working as a medical writer specializing in health promotion, fitness and anti-aging.
She is currently in the process of writing a book on testosterone, covering health related issues for both men and women.
———————————————————————————————————————————————–
References:
1. Castelli WP, Anderson K, Wilson PW, Levy D. Lipids and risk of coronary heart disease. The Framingham Study. Annals of epidemiology. Jan-Mar 1992;2(1-2):23-28.
2. Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science. Apr 4 1986;232(4746):34-47.
3. Castelli WP, Anderson K. A population at risk. Prevalence of high cholesterol levels in hypertensive patients in the Framingham Study. The American journal of medicine. Feb 14 1986;80(2A):23-32.
4. Superko HR. Did grandma give you heart disease? The new battle against coronary artery disease. The American journal of cardiology. Nov 5 1998;82(9A):34Q-46Q.
5. Freedman DS, Croft JB, Anderson AJ, et al. The relation of documented coronary artery disease to levels of total cholesterol and high-density lipoprotein cholesterol. Epidemiology. Jan 1994;5(1):80-87.
6. Grover SA, Coupal L, Hu XP. Identifying adults at increased risk of coronary disease. How well do the current cholesterol guidelines work? JAMA : the journal of the American Medical Association. Sep 13 1995;274(10):801-806.
7. Packard CJ, Shepherd J. Lipoprotein heterogeneity and apolipoprotein B metabolism. Arteriosclerosis, thrombosis, and vascular biology. Dec 1997;17(12):3542-3556.
8. Cromwell WC, Otvos JD, Keyes MJ, et al. LDL Particle Number and Risk of Future Cardiovascular Disease in the Framingham Offspring Study – Implications for LDL Management. Journal of clinical lipidology. Dec 2007;1(6):583-592.
9. Austin MA, Breslow JL, Hennekens CH, Buring JE, Willett WC, Krauss RM. Low-density lipoprotein subclass patterns and risk of myocardial infarction. JAMA : the journal of the American Medical Association. Oct 7 1988;260(13):1917-1921.
10. Lamarche B, Lemieux I, Despres JP. The small, dense LDL phenotype and the risk of coronary heart disease: epidemiology, patho-physiology and therapeutic aspects. Diabetes & metabolism. Sep 1999;25(3):199-211.
11. Sniderman AD, Blank D, Zakarian R, Bergeron J, Frohlich J. Triglycerides and small dense LDL: the twin Achilles heels of the Friedewald formula. Clinical biochemistry. Oct 2003;36(7):499-504.
12. Wang TY, Haddad M, Wang TS. Low triglyceride levels affect calculation of low-density lipoprotein cholesterol values. Archives of pathology & laboratory medicine. Mar 2001;125(3):404-405.
13. Ahmadi SA, Boroumand MA, Gohari-Moghaddam K, Tajik P, Dibaj SM. The impact of low serum triglyceride on LDL-cholesterol estimation. Archives of Iranian medicine. May 2008;11(3):318-321.
14. Lamarche B, Tchernof A, Moorjani S, et al. Small, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men. Prospective results from the Quebec Cardiovascular Study. Circulation. Jan 7 1997;95(1):69-75.
15. Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with risk for cardiovascular disease? Current atherosclerosis reports. Oct 2008;10(5):377-385.
16. Davidson MH, Ballantyne CM, Jacobson TA, et al. Clinical utility of inflammatory markers and advanced lipoprotein testing: advice from an expert panel of lipid specialists. Journal of clinical lipidology. Sep-Oct 2011;5(5):338-367.
17. Grundy SM, Vega GL, Tomassini JE, Tershakovec AM. Comparisons of apolipoprotein B levels estimated by immunoassay, nuclear magnetic resonance, vertical auto profile, and non-high-density lipoprotein cholesterol in subjects with hypertriglyceridemia (SAFARI Trial). The American journal of cardiology. Jul 1 2011;108(1):40-46.
18. McLaughlin T, Reaven G, Abbasi F, et al. Is there a simple way to identify insulin-resistant individuals at increased risk of cardiovascular disease? The American journal of cardiology. Aug 1 2005;96(3):399-404.
19. Sniderman AD. Differential response of cholesterol and particle measures of atherogenic lipoproteins to LDL-lowering therapy: implications for clinical practice. Journal of clinical lipidology. Feb 2008;2(1):36-42.
20. Faghihnia N, Tsimikas S, Miller ER, Witztum JL, Krauss RM. Changes in lipoprotein(a), oxidized phospholipids, and LDL subclasses with a low-fat high-carbohydrate diet. Journal of lipid research. Nov 2010;51(11):3324-3330.
21. Krauss RM. Dietary and genetic probes of atherogenic dyslipidemia. Arteriosclerosis, thrombosis, and vascular biology. Nov 2005;25(11):2265-2272.
22. Dreon DM, Fernstrom HA, Miller B, Krauss RM. Low-density lipoprotein subclass patterns and lipoprotein response to a reduced-fat diet in men. The FASEB journal : official publication of the Federation of American Societies for Experimental Biology. Jan 1994;8(1):121-126.
23. Parks EJ, Hellerstein MK. Carbohydrate-induced hypertriacylglycerolemia: historical perspective and review of biological mechanisms. The American journal of clinical nutrition. Feb 2000;71(2):412-433.
24. Kasim-Karakas SE, Lane E, Almario R, Mueller W, Walzem R. Effects of dietary fat restriction on particle size of plasma lipoproteins in postmenopausal women. Metabolism: clinical and experimental. Apr 1997;46(4):431-436.
25. Maki KC, Van Elswyk ME, McCarthy D, et al. Lipid responses to a dietary docosahexaenoic acid supplement in men and women with below average levels of high density lipoprotein cholesterol. Journal of the American College of Nutrition. Jun 2005;24(3):189-199.
26. Neff LM, Culiner J, Cunningham-Rundles S, et al. Algal docosahexaenoic acid affects plasma lipoprotein particle size distribution in overweight and obese adults. The Journal of nutrition. Feb 2011;141(2):207-213.







Thanks for this. This is by far the best explanation of blood cholesterol testing and its meaning that I have ever read.
I’m glad you find it informative.
At the risk of adding another me too comment, this was very good work, thank you. I’m always impressed & appreciative of those ‘flexing their intellect’ – not surprised to find it here on Will’s site. Please update me when the website and/or book is ready.
We gotta exercise or intellects as we do our muscles, in order to combat the invisible age-related deterioration.
Yes, here on the BZ you get to enjoy the products of that. Kudos to Will for having put together such a great resource:)
We aims to please 🙂
🙂 🙂
Hi Monica, thanks for an interesting and highly informative article. Do you know where a VAP test can be done in the UK if my GP does not offer it? The link in your article is for a USA provider. Regards, Gary
I’d suggest you ask your doctor about it.
Thank you very much for the excellent, pertinent and important imformation!!!!!!!
I’m glad you guys find it informative. 🙂
Excellent. The article clearly demonstrates the need for each person to take control of all phases their health. This is accomplished in part through education and information. The article was very informative and timely in preparing me for discussions with my doctor. Thank you.
I’m glad it came in handy for you. 🙂
Monica,
Thank you for the article on cholesterol. I’m reading it two days after my Dr. urged me to go on statins. I declined, wanting to do research to make an informed decision. I learned more from you in this single article than I did in two days of my own research. You are awesome.
Barbara
That’s great you refused statins. There are other much better and healthier ways to manage blood lipids.
This is a great Ariticle Monica. It is obvious that you did a lot of research to prepare a piece that we can all understand.
I have a question. what can one do to change the particle size of thier ldl if they discover that they have a type B profile?
I have always had high total cholesteral, with HDL being the prime contributor. my HDL/LDL ratio has always been good. now you have motivated me to find out what is going on with the LDL make-up.
The most effective way to improve the LDL makeup, ie to increase the LDL particle size and convert from type B to type A is to supplement with a high dose niacin (aka vitamin B3), 1000-3000 mg/day. However, make sure to get the regular niacin that causes flushing, and not slow-release (which is hepato-toxic, ie, damages the liver).
High dose niacin will also further elevate your HDL, which is a good thing.
The only drawback with high dose niacin is the flushing. Start taking 1000 mg (1g) after a meal and don’t leave the house for the next hours, because your skin will turn read like a tomato and you will feel like you’re on fire. This is a normal response; while uncomfortable, it’s not dangerous. And you will develop tolerance to this flushing as you keep taking it. So start with 1 g and progressively build up the dose to 2 or 3 g as your tolerance develops.
Oh God 🙂 it brings painful memories 🙂
I was then bulking and taking Niacin; It went from forehead slowly to knees …almost 2hours slow body travel
While there is certainly a lot of info in this article that impresses people, I believe it would have been written entirely differently if the author had read authors such as Uffe Ravnskov and Malcolm Kendrick, who both (separately) wrote a book entitled ‘The Great Cholesterol Con’. Reading Mary Enig’s work on fats and cholesterol will also assist.
A brief (?) summary of the above is as follows: your cholesterol level is irrelevant. People with every different level of cholesterol die of heart disease, because cholesterol doesnt cause heart disease. There is no such thing as a ‘bad’ cholesterol molecule (or lipoprotein) – its all there for a reason. The statements above that “Smaller LDL particles are more dangerous than the larger ones because they can more easily squeeze through the endothelium (a single cell layer that lines blood vessels) and clog up the artery walls. Smaller LDL particles also are more easily oxidized, and oxidized LDL is a significant contributor to the formation of plaques in the arteries.” are incorrect, because there is no known mechanism for cholesterol to ‘squeeze through the endothilium’, and any type of cholesterol, oxidised or otherwise, do not CAUSE plaques in the arteries. They are present but are not the original culprit.
Arteries become inflamed due to chronic stress (the stress hormone cortisol) and overconsumption of sugar and processed foods, trans fats, and industrially processed vegetable oils.(Note that saturated fats are NOT mentioned here – they are perfectly healthy). Cholesterol (your body’s building and repair molecule) is deposited there by the blood supply that feeds your artery walls in an attempt to fix the problem. Chronic inflammation leads to an accumulation of choleserol and other products that constrict the blood flow, but that isn’t the killer problem, becasue your arteries simply expand to restore blood flow. Damage to the endothilium in the inflamed and swollen areas causes blood to clot there in an attempt to repair it, and if these blood clots break loose, they can lodge elsewhere and cause myocardial infarction (one flavour of ‘heart attack’), or stroke.
This is one of the reasons statins dont actually reduce fatality (except in an extremely narrow class of patient, and then not by very much) – they artificially lower blood cholesterol when that was never the cause of the problem. Statins are associated with fatality by other causes (called ‘total mortality’ in the studies), but you dont hear about that. The main reason is, they are getting rid of the cholesterol your body needs to keep itself going.
In short, the best thing you can do for your health, and avoid all the confusing scientific-sounding mumbo jumbo, is eat REAL food, ignore your cholesterol level, and take a more relaxed approach to life. First read the above authors so you know exactly what I have been trying to get across.
Interesting. I’ve read some of this before. What’s your opinion on “today’s” saturated fats? Sure, there seems to be a lot of disagreement on whether saturated fats contribute to, or can exasperated CAD, but I’ve also read that because our livestock is fed with feed so very different then just 50 years ago, feed these animals were not naturally intended to eat, such GMO grains, soy, corn, wheat, discarded snack food waste, etc., that the chemical makeup of the fats in their meat have changed. We’re not only what we eat, we are what the animals we eat have eaten. Thanks in advance.
In the context of an unprocessed diet that doesn’t provide an excessive amount of carbs, saturated fats are perfectly fine and contributes to a healthy diet.
It is true today’s livestock is fed with less nutritious feed, and that meat and milk today is of lower quality than that of wild animals. This makes it even more important for us to cover the nutrient losses by making sure the other foods we eat, and our diet as a whole, provides us with all the nutrients we need, in the amounts we need.
Tim, I have read the books and papers by these authors and others, and need to correct your summary; it is your total LDL cholesterol level that is irrelevant. There are many other factors besides LDL that can jeopardize ones health.
And regarding your statement “there is no known mechanism for cholesterol to squeeze throuagh the endothelium”, please note that it is not the cholesterol to squeeze through, but the lipoproteins and their associated molecules (eg Apo B). You obviously have’t read the research studies
Yes, unprocessed foods and fats, including saturated fats, should be staple in every health promoting diet, and replace sugars and excessive amounts of carbs. It’s endothelial dysfunction that is the precursor of atherosclerosis and vascular senescence, and it has many causes, some of which you mention. High blood pressure is also an important culprit.
Arteries lose their functional and regenerative capacity because of circulating inflammatory mediators and other endogenous substances like ADMA etc that alter the balance between vasoconstricting and vasodilating molecules. Therefore, arteries don’t just simply “expand to restore blood flow” like you say. If it was that easy there wouldn’t be so many people suffering in today’s society.
Also, I want to say that it is not true that “the best thing you can do for your health is to avoid scientific mumbo jumbo”! Just telling people to eat “real foods” won’t do much good, as if you ask 10 different people what are real foods, you get 10 different answers.
The best thing you can do for your health is to get a good grasp on your current health status, by way of doing regular blood work to monitor risk factors, and to understand how your lifestyle, which includes food, exercise and relaxation, impacts your health. My mission with my writing is to help my readers with this understanding, and give advice on preventive measures.
Hi Monica,
I very much like your informative articles on the Brinkzone and your mission.
After regaining my health I built my own coaching business for helping people who have gotten themselves off track.
I’d love to add a link to this great article in my blog where I cover cholesterol.
Best regards from the UK,
Matt
Matt, I’m glad to hear that. And I admire your helping people, like myself.
Feel free to link to my article; and please email me the link to your blog. Thanks.
Great Article Monica. People are victims of a cholesterol hysteria and think that the lower the overall number or ldl the better. If they’re in that safe “range” they feel ok. As you pointed out it’s a false sense of security and overlooks the fact that cholesterol is a vital chemical for the body! Thanks Monica!
Yes, I’m on a mission to debunk the cholesterol and fat intake myths! Let’s spread the word 🙂
Hi Does anyone know where a VAP test can be done in the UK. You would not believe how far behind we are over here. Our medical system is still telling the public to eat low fat high carb and that Cholesterol causes heart disease
I sympathize with you; I am from Sweden myself and had this discussion with my mother when I tried to get her to run an advanced lipid panel. And yes, EU is sadly far behind the US. But lets hope that will chance in the not too distant future…
Its worse than you think. I have asked two Cardio’s and two GP’s and one nutritionist about where one can get an LDL particle size test done. None of them knew what the hell I was talking about. I am not kidding, they had not heard of LDL particle size and its possible relevance. Doctors here in the UK are kept in a very tight tunnel of information which is controlled by a body called N.I.C.E. Of course you can imagine who controls N.I.C.E. So this is one situation where you really dont want a NICE doctor.
It is sad that government censors health practices like that. I’d suggest you keep insisting and find a doctor who goes against the old med school dogma and narrow-mindedness.