In part 1 I introduced the new healthcare model called anti-aging medicine, and issues with the current disease oriented medical system that anti-aging medicine aims to solve. Here you will learn more about anti-aging medicine as a new medical specialty, how it differs from traditional medical practice, and what anti-aging qualified doctors can do for you.
What are Americans most concerned about when getting old?
According to a poll conducted by ABC News/USA Today, the most prominent concerns about aging are 78: * Losing one’s health 73%
* Losing one’s health 73%
* Losing ability to care for oneself 70%
* Losing mental abilities 69%
* Not being able to drive/travel on one’s own 59%
* Being a burden on one’s family 54%
* Winding up in a nursing home 52%
* Not being able to work or volunteer 49%
Amidst the epidemic of chronic diseases, it is not surprising that the top concern about aging include poor health, being unable to care for yourself and losing mental acuity. People are increasingly turning to anti-aging doctors for answers to these health concerns.
Insufficient clinical training in traditional medical school
The disease-based model of healthcare has significantly influenced medical school curricula 79. More medical students believe lifestyle changes are important when they begin medical school than when they finish 80. This shows the negative impact the current curricula have on the motivation of future healthcare providers regarding lifestyle behaviors 80-82.
The American Board of Medical Specialties lists 24 specialties and 121 subspecialties; integrating knowledge from these fields into a disease prevention/anti-aging curriculum would be overwhelming 83. Education on preventive medicine is widely considered inadequate, and there is little, if any, attention paid to health promotion or prescribing physical activity 84, 85. This was underscored by a study that investigated the views of leaders in academic medicine concerning the need for programs in preventive medicine and the prevailing barriers to program development 85. It was found that: – 91% considered academic preventive medicine underdeveloped.
– 91% considered academic preventive medicine underdeveloped.
– 100% considered their own programs average or worse.
– 80% perceived a shortage of preventive medicine faculty.
– 60% considered preventive medicine research quality to be inadequate.
Identified barriers to development and advancement of preventive medicine included funding constraints, academic bias to biomedicine, inadequate quality of preventive medicine research and faculty, preferences for technologic care, and the organization of academic medical centers. It was concluded that overcoming these barriers would require a change in our understanding of the tremendous role of prevention for improving health across the lifespan 85.
Medical students acquire sparse knowledge about prevention, and they see this field as an unappealing career choice, in large part due to the sparse funding in the area compared to well established medical specialties 83, 86. The importance of including the subject of preventive medicine in medical degree programs has been internationally recognized and has led to a number of initiatives to improve the incorporation of prevention into routine healthcare 87. The most well-known organization dedicated to help implement preventive medicine into the medical system is The American Academy of Anti-Aging Medicine, a.k.a. A4M.
What is Anti-Aging Medicine?
Motivated by discouraging disease trends, and guided by scientific research advances in our understanding of the mechanisms and causes behind chronic age-related diseases, The American Academy of Anti-Aging Medicine (A4M) was developed.
Anti-aging medicine is a relatively new, but quickly growing, medical specialty founded and led by A4M, with the mission, as stated on their website http://www.antiagingage.com/about/about-a4m, is:![]() “To advance technology and implement practices to detect, prevent, and treat aging related disease and to promote research into mechanisms and interventions to retard and optimize the human aging process.
“To advance technology and implement practices to detect, prevent, and treat aging related disease and to promote research into mechanisms and interventions to retard and optimize the human aging process.
The American Academy of Anti-Aging is also dedicated to educating physicians, scientists, and members of the public on biomedical sciences, breaking technologies, and anti-aging issues. The American Academy of Anti-Aging believes that the disabilities associated with normal aging are caused by physiological dysfunctions which in many cases can be prevented or improved by lifestyle and/or medical interventions.
In this way, The American Academy of Anti-Aging Medicine posits that chronological age and biological age do not have to coincide, and that both the human lifespan and health span can be increased as people grow older chronologically.
The American Academy of Anti-Aging seeks to disseminate information about innovative science and research, as well as treatment modalities designed to prolong and improve the human lifespan.
Anti-Aging Medicine is based on the scientific principles of evidence based medicine. Although The American Academy of Anti-Aging disseminates information on many types of medical treatments, it does not promote or endorse any specific treatment nor does it sell or endorse any commercial product.”
Thus, the mission of The American Academy of Anti-Aging Medicine (A4M) is essentially to help people live healthier and happier for longer. By compressing morbidity that arises from chronic lifestyle related diseases, which currently account for the majority of both premature and late-life mortality, A4M makes the case that increasing healthspan will also increase life span and the years spent living in youthful vigor.
What distinguishes doctors who practice Anti-Aging Medicine under the guidance of A4M?
A4M emphasizes individualized care; this is evident from the first visit, with A4M board certified doctors reporting that they spend between two and five hours with new patients 88. A4M doctors are less concerned about assigning a disease label to a patient’s problems than they are about uncovering its causes and underlying processes. They see “the patient who has the disease” not “the disease of the patient”. In line with this, they take extensive lifestyle histories that include things traditional medicine often neglects, such as nutrition, exercise, sleep habits, supplements, stress etc.
Here are two insightful quotes from interviews with A4M doctors 88:
“We spend more time with our patients. We dig a little deeper. We’re looking at the whole person…. A lot of conventional doctors would say ‘Well it’s in range, you’re fine’. We look beyond the ‘normal’ ranges and look for the optimal ranges. So we’re kind of focused more on optimal health, versus just normal, and on treating the underlying cause instead of just matching a drug with the bug.”
“We look at the whole person, all of the disease processes put together and trying to find out what is the core reason and what are the causative factors, whereas in conventional medicine we all work in a silo. I mean the orthopedists do theirs, and somebody’s got a foot specialist and a hand specialist and an ear specialist, and right now current medicine is fragmental where doctors do their own thing. We try to put all those pieces of the puzzle together.”
This emphasis on “optimal health” instead of just “normal” is the reason anti-aging medicine doctors see themselves as being in the vanguard of medicine 88, 89. Their goal is to create optimal functioning, and not be satisfied when tests and functioning falls within “normal” ranges defined statistically. Anti-aging medicine doctors also prefer to define “normal” ranges based on the individual patient in question, in order to improve the patient’s health and achieve an optimal state of being that is individually defined. They see their patients as unique individuals and not as the mean in a graph of statistical dots.
Anti-aging medicine doctors reject the traditional “disease model” of medicine – which that focuses on standardized measures and tests and on uniform diagnoses – in favor of strategies that allow them to gain a deeper perspective on why patients have particular symptoms. The modes of treatment they choose are preventive ones. For example, if a patient presents with blood sugar levels in the upper end of the “normal” range, the anti-aging medicine doctor will educate the patient on the importance of exercise and proper nutrition, instead of saying “your level is within range, you’re fine” and wait for diabetes to develop, at which point they simply prescribe a medication.
This is illustrated by another insightful quote from an A4M doctor 88:
“There is minimal emphasis on prevention in medical school. … no one cares about it and typical doctors don’t know much about it. They are a lot more interested in learning how to do a bypass surgery than they are in what the optimal dose of calcium is to prevent osteoporosis, how exercise can improve cardiovascular system etc, and things along those lines.”
Primary Prevention – the future of medicine and healthspan extension
As outlined above, A4M certified doctors embrace the power of primary prevention, e.g. strategies that prevent the development of diseases in the first place. Primary prevention keeps the disease process from becoming established by eliminating causes of disease and/or by increasing resistance to disease 90, 91. Anti-aging doctors fill a void in wellness-oriented preventive healthcare that is sought by an increasingly greater segment of the population as it ages 92.
Figure 1 below nicely illustrate the essence of anti-aging medicine; from longer life span to longer health span (and life span) 93.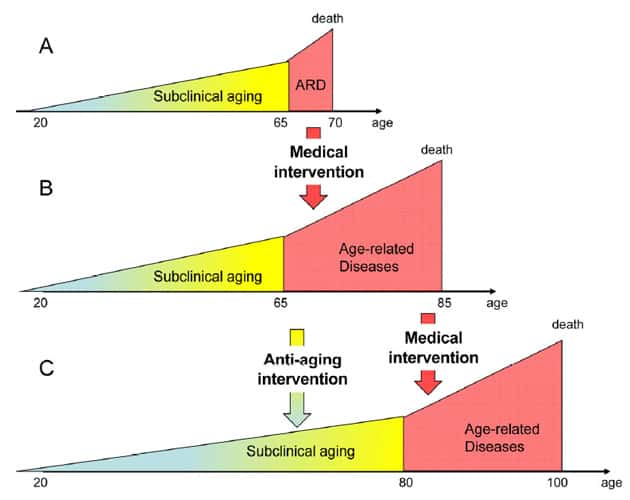
Figure 1
From A to B: Standard medicine increases lifespan by preventing death from age‐related diseases. It simultaneously increases a number of old people suffering from age‐related diseases.
From B to C: Anti‐aging interventions will slow down processes that contribute to physiological declines associated with chronological aging, and delay the onset of age‐related diseases.
With progress in preventive and anti-aging medicine, and in helping people make lifestyle changes, the red area in the figure “age-related diseases” will become an even smaller part of the total lifespan due to compression of morbidity and consequent increases in healthspan 91, 94-97. This is illustrated in figure 2 91:
Figure 2
Scenarios for future morbidity. Shaded areas represent cumulative morbidity.
(1) Present morbidity
(2) Life extension; a future where both life expectancy and morbidity are both increased
(3) Compression of Morbidity; a future where onset of morbidity is delayed, and lifespan in increased, resulting in Compression of Morbidity and an increase in healthspan.
Proof that compression of morbidity is possible in reality comes from several studies of exceptional longevity in centenarians (people over 100 years old) 98-101. Super-centenarians (those over age 105) have proved to have had less lifetime cumulative morbidity than those dying at age 85 or 100 98. This suggests that a healthy lifestyle that prevents onset of chronic diseases and morbidity can help everybody increase both their lifespan and healthspan.
Further proof that is it unhealthy lifestyles, and not the biological aging process, that cause impairments to physical performance that commonly start to manifest in middle age, comes from studies of master athletes 102, 103. For example, it has been found that 25% of the 65-69 year old runners were faster than 50% of the 20-54 year old runners 102. This survey also revealed that more than 25% of the 50-69 year-old runners had started their marathon training only in the past 5 years 102. Thus, performance losses in middle age are mainly due to a sedentary lifestyle, rather than biological aging. This shows that even at an advanced age non-athletes can achieve high levels of performance through regular training.
Researchers have suggested that centenarians and master athletes are ideal models for studying healthy/successful aging and search for clues that can help everybody age well 99-101, 104, 105. These populations show us that the aging process is modifiable, and that healthspan extension is a viable option for everybody to pursue via daily lifestyle choices.
Summary
In stark contrast to traditional medicine, which focuses on treatment of diseases and disturbed health 1, 106, the main objective of anti-aging medicine is health promotion and disease prevention, primarily through healthy lifestyles with regular exercise/physical activity and proper nutrition.
Anti-Aging Medicine is the fastest-growing medical specialty throughout the world. The specialty was originally developed by The American Academy of Anti-Aging Medicine (A4M), and is founded on the application of advanced scientific technologies for the early detection, prevention, treatment and reversal of age-related dysfunction, disorders and diseases. It is a health care model promoting innovative science and research to prolong the healthy lifespan in humans.
The term “anti-aging” relates to the application of advanced biomedical technologies focused on the early detection, prevention and treatment of aging-related disease. The goal of anti-aging is not to merely to prolong the total years of an individual’s life, but to ensure that those years are enjoyed in a healthy, productive and vital state.
In the US, over 85% of our health care dollars go to treatment of chronic lifestyle induced diseases. These persistent conditions – the nation’s leading causes of death and disability – cause deaths that could have been prevented, lifelong disability, compromised quality of life, and burgeoning health care costs.
Guided by advances in health promotion and medical research, A4M encourages doctors to personalize treatments based on every patient’s unique circumstances, and not succumb to statistically driven medical decision making, which characterizes the current medical system.
A4M also encourages people to learn about their health status and risks factors. Asymptomatic diseases or risk factors for non-communicable diseases are extremely frequent among the general population 107. And most people are not sufficiently aware of their health risks to act up and change their lifestyle and take appropriate preventive measures 107. By becoming actively involved in improving ones health by making healthy lifestyle choices, everybody can take personal control over their health and aging destiny.
References:
78. Today AN-U. Poll: Living Longer, Living Better. In October 16, (Ed). http://abcnews.go.com/images/Politics/995a1Longevity.pdf 2006.
79. Abrahamson S. Time to return medical schools to their primary purpose: education. Academic medicine : journal of the Association of American Medical Colleges. 1996;71(4):343-347.
80. Frank E, Tong E, Lobelo F, et al. Physical activity levels and counseling practices of U.S. medical students. Medicine and science in sports and exercise. 2008;40(3):413-421.
81. Lobelo F, Duperly J, Frank E. Physical activity habits of doctors and medical students influence their counselling practices. British journal of sports medicine. 2009;43(2):89-92.
82. Moynihan R. Doctors’ education: the invisible influence of drug company sponsorship. BMJ. 2008;336(7641):416-417.
83. Matheson GO, Klugl M, Dvorak J, et al. Responsibility of sport and exercise medicine in preventing and managing chronic disease: applying our knowledge and skill is overdue. British journal of sports medicine. 2011;45(16):1272-1282.
84. Mohler MJ, D’Huyvetter K, Tomasa L, et al. Healthy aging rounds: using healthy-aging mentors to teach medical students about physical activity and social support assessment, interviewing, and prescription. Journal of the American Geriatrics Society. 2010;58(12):2407-2411.
85. Gottlieb LK, Holman HR. What’s preventing more prevention? Barriers to development at academic medical centers. Journal of general internal medicine. 1992;7(6):630-635.
86. Brun D, Hassid S, d’Ivernois JF. [How do physicians evaluate their medical school training. Retrospective survey of 4 groups of medical students 8-11 years after graduation]. Presse Med. 1999;28(21):1121-1127.
87. Pomrehn PR, Davis MV, Chen DW, et al. Prevention for the 21st century: setting the context through undergraduate medical education. Academic medicine : journal of the Association of American Medical Colleges. 2000;75(7 Suppl):S5-13.
88. Fishman JR, Settersten RA, Jr., Flatt MA. In the vanguard of biomedicine? The curious and contradictory case of anti-ageing medicine. Sociology of health & illness. 2010;32(2):197-210.
89. Mykytyn CE. Anti-aging medicine: a patient/practitioner movement to redefine aging. Soc Sci Med. 2006;62(3):643-653.
90. Kones R. Is prevention a fantasy, or the future of medicine? A panoramic view of recent data, status, and direction in cardiovascular prevention. Therapeutic advances in cardiovascular disease. 2011;5(1):61-81.
91. Fries JF, Bruce B, Chakravarty E. Compression of morbidity 1980-2011: a focused review of paradigms and progress. Journal of aging research. 2011;2011:261702.
92. Klatz R. Anti-Aging medicine and why it must be part of your practice. http://www.chiroweb.com/mpacms/dc_ca/article.php?id=52406 2007.
93. Blagosklonny MV. Answering the ultimate question “what is the proximal cause of aging?”. Aging. 2012;4(12):861-877.
94. Vita AJ, Terry RB, Hubert HB, et al. Aging, health risks, and cumulative disability. The New England journal of medicine. 1998;338(15):1035-1041.
95. Hubert HB, Bloch DA, Oehlert JW, et al. Lifestyle habits and compression of morbidity. The journals of gerontology Series A, Biological sciences and medical sciences. 2002;57(6):M347-351.
96. Fries JF. Aging, natural death, and the compression of morbidity. The New England journal of medicine. 1980;303(3):130-135.
97. Kalache A, Aboderin I, Hoskins I. Compression of morbidity and active ageing: key priorities for public health policy in the 21st century. Bulletin of the World Health Organization. 2002;80(3):243-244.
98. Andersen SL, Sebastiani P, Dworkis DA, et al. Health span approximates life span among many supercentenarians: compression of morbidity at the approximate limit of life span. The journals of gerontology Series A, Biological sciences and medical sciences. 2012;67(4):395-405.
99. Willcox BJ, Willcox DC, Ferrucci L. Secrets of healthy aging and longevity from exceptional survivors around the globe: lessons from octogenarians to supercentenarians. The journals of gerontology Series A, Biological sciences and medical sciences. 2008;63(11):1181-1185.
100. Willcox DC, Willcox BJ, Wang NC, et al. Life at the extreme limit: phenotypic characteristics of supercentenarians in Okinawa. The journals of gerontology Series A, Biological sciences and medical sciences. 2008;63(11):1201-1208.
101. Engberg H, Oksuzyan A, Jeune B, et al. Centenarians–a useful model for healthy aging? A 29-year follow-up of hospitalizations among 40,000 Danes born in 1905. Aging cell. 2009;8(3):270-276.
102. Leyk D, Ruther T, Wunderlich M, et al. Physical performance in middle age and old age: good news for our sedentary and aging society. Deutsches Arzteblatt international. 2010;107(46):809-816.
103. Wang BW, Ramey DR, Schettler JD, et al. Postponed development of disability in elderly runners: a 13-year longitudinal study. Archives of internal medicine. 2002;162(20):2285-2294.
104. Hawkins SA, Wiswell RA, Marcell TJ. Exercise and the master athlete–a model of successful aging? The journals of gerontology Series A, Biological sciences and medical sciences. 2003;58(11):1009-1011.
105. Willcox DC, Willcox BJ, Poon LW. Centenarian studies: important contributors to our understanding of the aging process and longevity. Current gerontology and geriatrics research. 2010;2010:484529.
106. Singh AR. Modern Medicine: Towards Prevention, Cure, Well-being and Longevity. Mens sana monographs. 2010;8(1):17-29.
107. Keipes M, Bellucci A, Hansen E. Risk factors and disease prevalence in 3331 personal check-ups performed in preventive medicine between 2006 and 2011. cross-sectional and follow-up study. Bulletin de la Societe des sciences medicales du Grand-Duche de Luxembourg. 2012(2):25-35.






Thank you, Monica, for your articles (parts 1 and 2) on anti-aging medicine. Your articles are always so well thought out and well researched. Keep them coming. I have the utmost respect for you and Will Brink. And thank you for being so inspirational to me.